TL;DR:
- Clinical personalisation tailors mental health interventions to individual biological, psychological, and social factors rather than using standard protocols. It involves continuous adaptation based on personal data, preferences, and real-time assessments to improve outcomes. Integrating AI tools and comprehensive baseline evaluations enhances the effectiveness of personalized treatment approaches.
Clinical personalisation is the practice of adapting medical and therapeutic interventions to the unique biological, psychological, and social characteristics of each patient, rather than applying population-based protocols uniformly. For mental health professionals, this distinction matters enormously. A treatment plan built around a population average may miss the individual entirely. The shift toward tailored treatment plans grounded in personal baselines, psychosocial context, and real-time data is redefining what effective care looks like in 2026.
What is clinical personalisation in mental health care?

Clinical personalisation is defined as the continuous adaptation of clinical decisions to an individual's specific data profile, preferences, and circumstances across the full course of their care. The term is sometimes used interchangeably with "personalised medicine," but the two are distinct. Personalised medicine, as a recognised field, tends to focus on molecular and genomic data to guide drug selection. Clinical personalisation is broader. It encompasses psychosocial factors, lived experience, patient preferences, and dynamic reassessment over time.
This distinction matters most in mental health, where biological markers rarely tell the whole story. A patient's response to cognitive behavioural therapy depends not just on their diagnosis, but on their attachment history, social support, cultural background, and current life stressors. Patient-centred care that accounts for all these dimensions produces better outcomes than any single-variable model.
The concept also connects to what researchers call the "N-of-1" approach: using high-frequency individual data to optimise care for one person rather than a cohort. For mental health clinicians, this means tracking symptom trajectories, treatment responses, and contextual shifts over time to refine the therapeutic approach continuously.
How does clinical personalisation differ from precision medicine?
The terms clinical personalisation, precision medicine, and clinical customisation are often conflated. Each describes a related but distinct approach to improving care.
| Approach | Primary Focus | Data Sources | Mental Health Relevance |
|---|---|---|---|
| Precision medicine | Molecular subgrouping | Genetics, biomarkers, imaging | Limited; useful for pharmacogenomics |
| Clinical personalisation | Individual adaptation | Psychosocial, clinical history, preferences | High; central to therapeutic planning |
| Clinical customisation | Protocol adjustment | Workflow and procedural data | Moderate; supports delivery flexibility |
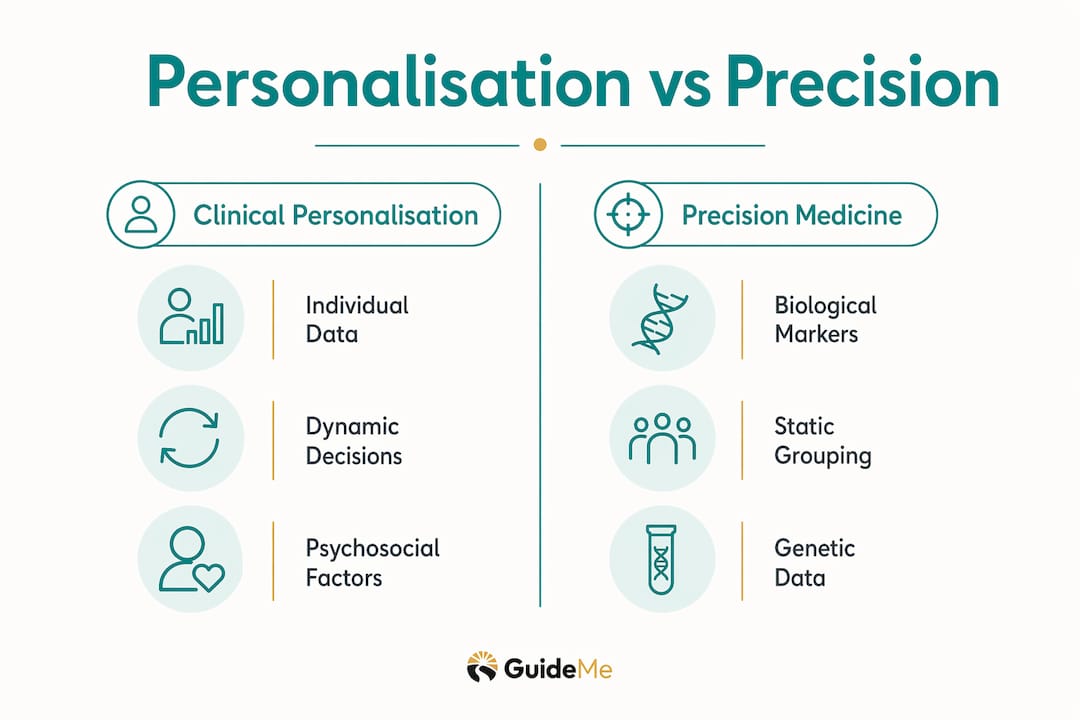
Precision medicine focuses on molecular data to subgroup patients for therapy, while clinical personalisation encompasses adapting treatment to psychosocial contexts and individual preferences. The two approaches are complementary, not competing. A psychiatrist might use pharmacogenomic data to select a medication, then apply clinical personalisation principles to adjust dosage, therapy modality, and session frequency based on the patient's ongoing response and life circumstances.
Clinical customisation sits closer to the operational layer. It refers to adjusting clinical protocols and workflows to fit a patient's specific needs, without necessarily changing the underlying treatment logic. Key distinctions worth noting:
- Precision medicine asks: "Which subgroup does this patient belong to?"
- Clinical personalisation asks: "What does this specific individual need right now?"
- Clinical customisation asks: "How do we deliver that care in a way that fits this patient's context?"
For mental health researchers, the implication is clear. Biological subgrouping alone will not capture the complexity of conditions like depression, anxiety, or trauma. Effective personalised care in this field requires integrating biological data with psychosocial assessment and continuous clinical dialogue.
How is AI transforming clinical personalisation in mental health?
AI is accelerating clinical personalisation by enabling clinicians to synthesise far more patient data than any manual review process could handle. AI-driven personalisation in 2026 integrates genetics, clinical history, imaging, and lifestyle data to refine diagnostics and treatment selection. The practical applications in mental health are growing rapidly.
Current AI applications relevant to mental health personalisation include:
- Symptom pattern recognition across longitudinal data to detect early relapse signals
- Treatment response prediction using prior therapy outcomes and patient characteristics
- Adaptive assessment tools that adjust question sets based on prior responses
- Clinical decision support that surfaces relevant risk factors during consultations
Despite this promise, high implementation costs and workforce skill deficits remain the primary barriers limiting clinical adoption. Many mental health services lack the infrastructure to collect, store, and analyse the data volumes that AI tools require. Clinicians also need training not just in using these tools, but in interpreting their outputs critically.
Pro Tip: When reviewing AI-generated clinical recommendations, always cross-reference the output against your direct clinical observations. AI tools surface patterns in data; they do not account for what the patient told you in the room. Treat AI outputs as one input among several, not as a directive.
The most promising development for mental health practice is the emergence of causal digital twins: computational models that simulate how a specific patient might respond to different treatment options in real time. This moves beyond prediction toward genuine simulation, allowing clinicians to test therapeutic pathways before committing to them.
What are the evidence-based benefits of personalised clinical care?
The evidence base for clinical personalisation is growing, and the findings are compelling. A study of over 100 million lab tests in more than 800,000 patients demonstrated that personalised reference intervals predict morbidity and treatment outcomes more accurately than population-based standards. This finding has direct implications for mental health, where biomarker monitoring is increasingly used alongside psychological assessment.
The core mechanism is straightforward. Deviation from a personalised baseline provides stronger risk indicators than population intervals. A result that falls within the normal population range may still represent a significant shift for a specific individual. Catching that shift early changes the clinical picture entirely.
The documented benefits of adopting personalised approaches in mental health practice include:
- Improved treatment efficacy through better matching of therapy type to patient profile
- Reduced side effects in pharmacological treatment by accounting for individual metabolic variation
- Higher patient engagement when patients feel their care reflects their actual experience
- Earlier detection of deterioration through individual baseline monitoring
The practical challenges are real, however. Dynamic clinical personalisation requires decoupling decision logic from static workflows, which demands both technical infrastructure and a willingness to move beyond fixed protocols. Many mental health services still operate on standardised care pathways that leave little room for real-time adaptation.
Immunotherapy research offers a useful parallel. Understanding unique patient biology allows targeted treatments that enhance effectiveness and reduce harm to healthy tissue. The same logic applies in mental health: understanding the individual reduces therapeutic collateral damage and increases the precision of the intervention.
How can mental health professionals implement personalisation effectively?
Implementing clinical personalisation in a mental health setting requires a structured approach. The following steps provide a practical framework for clinicians and service leads.
-
Establish an individual baseline. Collect comprehensive intake data covering clinical history, psychosocial context, previous treatment responses, and patient preferences. This baseline becomes the reference point for all subsequent clinical decisions.
-
Select therapy modality based on the individual profile. Match the therapeutic approach to the patient's specific presentation, not just their diagnosis. A patient with complex trauma and a dismissive attachment style will not respond to the same CBT protocol as a patient with a single-episode depressive disorder.
-
Integrate dynamic assessment into the treatment plan. Use validated outcome measures at regular intervals to track individual response. Adjust the plan when the data indicates a shift, rather than waiting for a scheduled review.
-
Use modern EMR tools to support personalised workflows. Context-aware EMR systems now automatically adjust interfaces and prompts based on patient-specific data, reducing cognitive load and surfacing relevant clinical information at the right moment.
-
Maintain ongoing dialogue with the patient. Clinical personalisation is not a one-time assessment. It requires continuous collaboration between clinician and patient to ensure the plan reflects the patient's evolving needs and preferences.
Pro Tip: The most common failure point in personalised care is the initial assessment. Clinicians often collect rich data at intake and then revert to standard protocols. Build a formal review trigger into your treatment plan at weeks four and eight, so the data you collected actually informs ongoing decisions.
Exploring personalised medicine principles from adjacent healthcare fields can also strengthen your approach. Combining diverse health data sources, including biological, psychological, and social variables, produces a more complete picture of the individual than any single domain can provide.
Key takeaways
Clinical personalisation produces better mental health outcomes when it integrates individual baselines, psychosocial context, and dynamic reassessment rather than relying on population-level protocols.
| Point | Details |
|---|---|
| Definition clarity | Clinical personalisation adapts care to the individual; precision medicine subgroups by molecular data. |
| Individual baselines matter | Deviations from a personal baseline predict risk more accurately than population reference ranges. |
| AI as a clinical tool | AI synthesises complex patient data but requires critical interpretation alongside direct clinical observation. |
| Dynamic workflows are necessary | Effective personalised care requires moving beyond static protocols to real-time treatment adjustment. |
| Implementation starts at intake | Comprehensive baseline assessment is the foundation of any genuinely personalised treatment plan. |
From population averages to individual baselines: a practitioner's view
I have spent years watching mental health services default to population-level thinking, not because clinicians do not care about the individual, but because the systems they work within reward standardisation. Waiting list pressures, audit requirements, and commissioning frameworks all push toward the average. Clinical personalisation asks you to push back.
What strikes me most about the evidence emerging in 2026 is how clearly it demonstrates that the average is often the wrong answer. When a study of over 800,000 patients shows that individual baselines outperform population standards for predicting morbidity, that is not a marginal finding. It is a fundamental challenge to how we design care pathways.
The mental health field has always understood, at least in theory, that each patient is different. The gap has been between that understanding and the systems we build to deliver care. The N-of-1 approach, combined with context-aware EMR tools and AI-supported pattern recognition, is finally giving us the infrastructure to act on what we already know.
My honest view is that the biggest barrier is not technology. It is the clinician's willingness to treat the individual data in front of them as more authoritative than the protocol behind them. That is a training issue, a supervision issue, and a culture issue. Technology can support personalised care. It cannot create the clinical curiosity that makes it work.
Interdisciplinary collaboration is also underused. Psychiatrists, psychologists, social workers, and occupational therapists each hold different pieces of the individual picture. Personalised care that draws on all those perspectives is categorically more accurate than any single-discipline assessment.
— Yetty
How Guidemetherapy supports personalised therapy planning
Guidemetherapy is built on the same principles that make clinical personalisation effective: start with the individual, not the protocol.
The platform combines human clinical insight with AI-powered matching to create an in-depth therapy plan before a patient ever meets a therapist. That means the matching process accounts for the patient's specific presentation, preferences, and therapeutic history, rather than simply assigning the next available clinician. For mental health professionals who want their clients to arrive at therapy already oriented toward the right fit, Guidemetherapy offers a structured, patient-centred pathway that reduces the friction of getting started and increases the likelihood of a productive therapeutic relationship from the first session.
FAQ
What is clinical personalisation in mental health?
Clinical personalisation in mental health is the process of adapting therapeutic interventions to an individual's unique biological, psychological, and social profile. It moves beyond standard diagnostic protocols to account for personal history, preferences, and real-time clinical data.
How does clinical personalisation differ from precision medicine?
Precision medicine uses molecular and genetic data to subgroup patients for treatment, while clinical personalisation integrates psychosocial context, patient preferences, and dynamic reassessment. Both approaches improve care, but clinical personalisation is broader and more directly applicable to mental health practice.
What role does AI play in personalised mental health care?
AI supports clinical personalisation by synthesising large volumes of patient data to identify patterns, predict treatment responses, and support clinical decision-making. Current barriers include infrastructure costs and the need for clinician training in interpreting AI outputs critically.
What are personalised reference intervals and why do they matter?
Personalised reference intervals are individual-specific benchmarks derived from a patient's own historical data, rather than population norms. Research across more than 800,000 patients shows they predict morbidity and treatment outcomes more accurately than standard population-based ranges.
How can clinicians start implementing personalised care today?
Clinicians can begin by conducting comprehensive baseline assessments at intake that capture psychosocial context alongside clinical history, then building formal review points into treatment plans to ensure the data collected actively informs ongoing care decisions.